Controlled Substance Protocol
Walgreens's pharmacists need a method and process to ensure that any dispensed controlled substances comply with the Controlled Substance Protocol (CSP) and the Controlled Substances Act.
GOALS
Design a way for pharmacists to accept or decline a prescription that falls under the controlled substance protocol while ensuring each CSP prescription has a worksheet attached for audit and Controlled Substance Act regulations.
In addition, if the CSP prescription is incorrectly reviewed, implement an exception process to remove it from fulfillment, add the exception, and submit it for reprocessing. Lastly, provide a method worksheets can be saved and accessed by various team members with a documented history of previous worksheets.
CHALLENGES
Training a junior designer on the design system and processes and - mentoring them on the best design approach while performing design reviews for onshore and offshore teams (while doing my design tasks).
The documentation process for post-determining which prescriptions were accepted or rejected under CSP.
Determining which red flags and CRDs (control response determinations) apply to which team member.
Shifting team members away from their wayward thinking on CSP worksheets in the legacy system (a very outdated and convoluted process).
Eliminate duplicate records for when a pharmacist or technician edits a new worksheet for a CSP prescription.
MY ROLE
Build storyboards and medium wireframes to illustrate the professional services process.
Analyze and create multiple user flows for professional services (both desktop and mobile).
Create annotated wireframes and tab order diagrams for the engineering and elaboration process (for final implementation).
Design pixel-perfect high-fidelity wireframes for prototype and usability testing purposes.
As a senior designer, I lead a series of design reviews and office hours for onshore and offshore designers while completing my design-related responsibilities for this topic.
WHAT I DELIVERED
3 User flows
35 Medium-fidelity wireframes
1 Storyboard
30 High-fidelity wireframes
30 Annotated wireframes
6 Tab order diagrams
GOALS
Design a way for pharmacists to accept or decline a prescription that falls under the controlled substance protocol while ensuring each CSP prescription has a worksheet attached for audit and Controlled Substance Act regulations.
In addition, if the CSP prescription is incorrectly reviewed, implement an exception process to remove it from fulfillment, add the exception, and submit it for reprocessing. Lastly, provide a method worksheets can be saved and accessed by various team members with a documented history of previous worksheets.
CHALLENGES
Training a junior designer on the design system and processes and - mentoring them on the best design approach while performing design reviews for onshore and offshore teams (while doing my design tasks).
The documentation process for post-determining which prescriptions were accepted or rejected under CSP.
Determining which red flags and CRDs (control response determinations) apply to which team member.
Shifting team members away from their wayward thinking on CSP worksheets in the legacy system (a very outdated and convoluted process).
Eliminate duplicate records for when a pharmacist or technician edits a new worksheet for a CSP prescription.
MY ROLE
Build storyboards and medium wireframes to illustrate the professional services process.
Analyze and create multiple user flows for professional services (both desktop and mobile).
Create annotated wireframes and tab order diagrams for the engineering and elaboration process (for final implementation).
Design pixel-perfect high-fidelity wireframes for prototype and usability testing purposes.
As a senior designer, I lead a series of design reviews and office hours for onshore and offshore designers while completing my design-related responsibilities for this topic.
WHAT I DELIVERED
3 User flows
35 Medium-fidelity wireframes
1 Storyboard
30 High-fidelity wireframes
30 Annotated wireframes
6 Tab order diagrams
RESEARCH
DIFFERENT CONCEPT
This topic was not as large as some of the previous topics I had completed. Instead, it was more complex and required me to divide my time between mentoring, reviewing, and providing direction for other design topics. This topic discussed leveraging existing functionality in the legacy system and porting it into the UI with new specifications and improvements.
EXISTING SYSTEM
The legacy system was barebones in that a pharmacist or technician could perform minimal tasks when working on a CSP worksheet. They often performed the same action twice due to how the prescriptions were stored and processed under CSA regulation and were prone to audits. I wanted to understand more about the main pain points of the existing system. I spoke with SMEs and the PM about what was found during the workshops.


TOP PAIN POINTS
As a pharmacist or technician, I have to make duplicate records of a CSA resolution, often resulting in a loss of time for other pharmacy tasks.
As a pharmacist, I have no way of accepting or rejecting worksheets based on incorrect criteria in an existing worksheet. It is often confusing to understand which prescription it is attached to correct the mistake.
As a pharmacist, I cannot access previous CSA worksheet information. It is hard to ascertain who made what changes, when, and why until the point of sale, thus resulting in a large influx of worksheets to complete during patient interactions.
As a pharmacist, I have to add an exception to remove a CSA prescription from the fulfillment and submit it for reprocessing (based on the rule engine outlined in clinical interactions).
RESEARCH
DIFFERENT CONCEPT
This topic was not as large as some of the previous topics I had completed. Instead, it was more complex and required me to divide my time between mentoring, reviewing, and providing direction for other design topics. This topic discussed leveraging existing functionality in the legacy system and porting it into the UI with new specifications and improvements.
EXISTING SYSTEM
The legacy system was barebones in that a pharmacist or technician could perform minimal tasks when working on a CSP worksheet. They often performed the same action twice due to how the prescriptions were stored and processed under CSA regulation and were prone to audits. I wanted to understand more about the main pain points of the existing system. I spoke with SMEs and the PM about what was found during the workshops.
TOP PAIN POINTS
As a pharmacist or technician, I have to make duplicate records of a CSA resolution, often resulting in a loss of time for other pharmacy tasks.
As a pharmacist, I have no way of accepting or rejecting worksheets based on incorrect criteria in an existing worksheet. It is often confusing to understand which prescription it is attached to correct the mistake.
As a pharmacist, I cannot access previous CSA worksheet information. It is hard to ascertain who made what changes, when, and why until the point of sale, thus resulting in a large influx of worksheets to complete during patient interactions.
As a pharmacist, I have to add an exception to remove a CSA prescription from the fulfillment and submit it for reprocessing (based on the rule engine outlined in clinical interactions).
PLAN
WORKFLOW
As a next step, the goal was to create user flows for each defined use case. The process follow my previous approach of building out a workflow for a single use case or group of use cases that helped visualize the workflow for the controlled substance protocol.
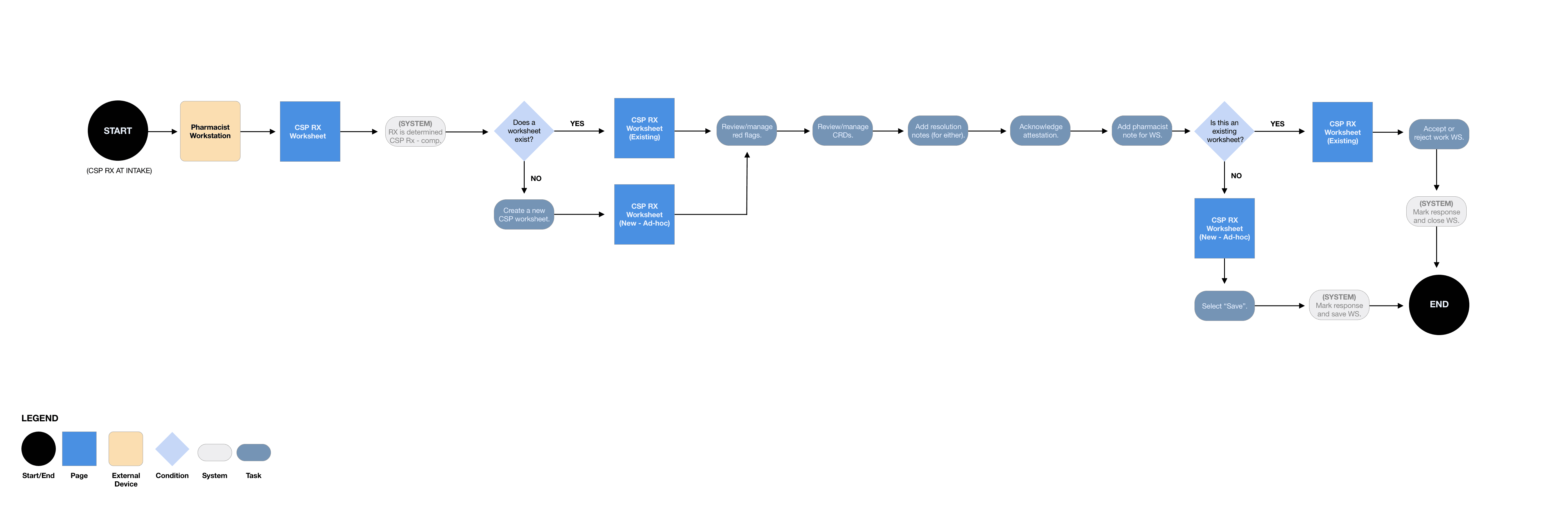
CSP - COMPLETE WORKSHEET (RPH)
The first workflow I constructed showed how a pharmacist would complete an existing worksheet or create a new one with a CSP prescription and tie it to a worksheet. CSA regulations required a physical or digital attachment when dispensing a scheduled class drug. CSP regulations were adhered to by having the pharmacist review the red flags and CRDs, acknowledge through attestation and pharmacist notation. The new process allowed them to save it (should it need to be designed later or required to follow), accept or reject and close the worksheet for final dispense to the patient.
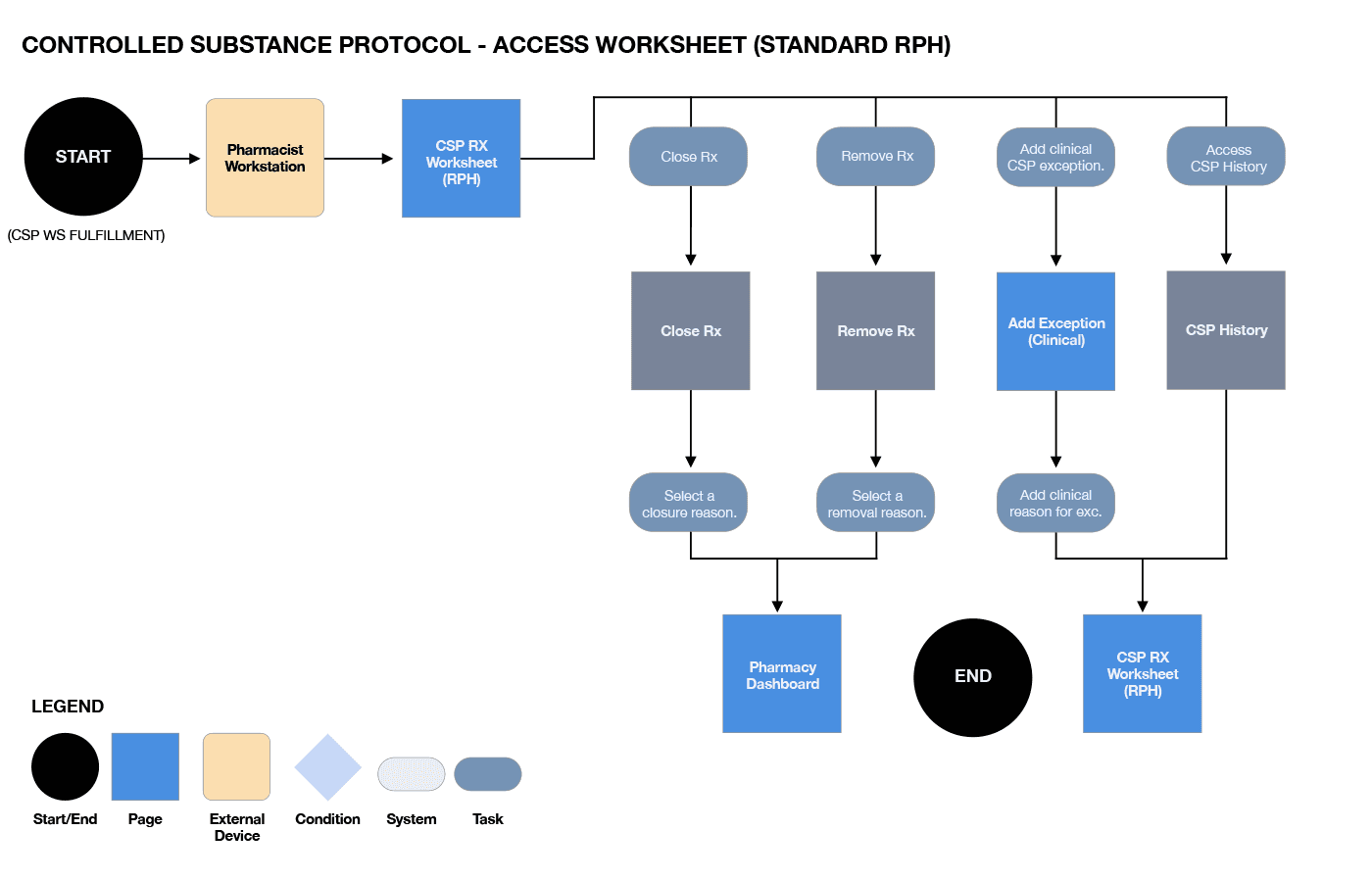
CSP - ACCESS EXISTING WORKSHEET (RPH)
I constructed the following workflow that showed how a pharmacist could access an existing worksheet another pharmacist previously worked on; they could also continue working on this worksheet and remove, close, or add an exception for this prescription. In addition, access CSP history for this prescription to understand the previous pharmacist discussions about it and external audit purposes.
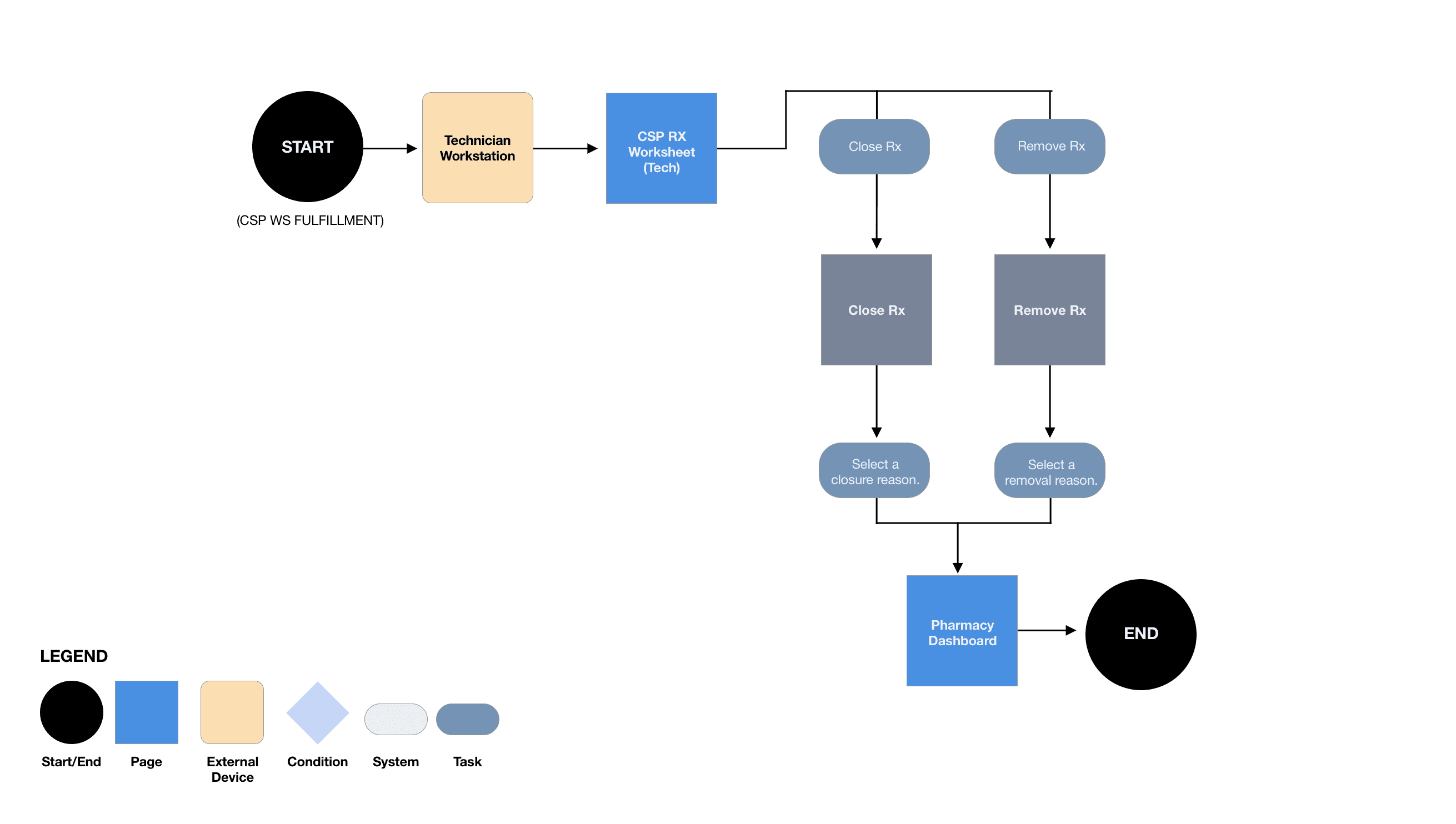
CSP - ACCESS EXISTING WORKSHEET (TECHNICIAN)
The last workflow I constructed showed how a technician could access an existing worksheet another technician or pharmacist previously worked on. In addition, they could continue working on this worksheet and save any required adjustments to the worksheet. A technician could not accept or reject a worksheet.
PLAN
WORKFLOW
As a next step, the goal was to create user flows for each defined use case. The process follow my previous approach of building out a workflow for a single use case or group of use cases that helped visualize the workflow for the controlled substance protocol.
CSP - COMPLETE WORKSHEET (RPH)
The first workflow I constructed showed how a pharmacist would complete an existing worksheet or create a new one with a CSP prescription and tie it to a worksheet. CSA regulations required a physical or digital attachment when dispensing a scheduled class drug. CSP regulations were adhered to by having the pharmacist review the red flags and CRDs, acknowledge through attestation and pharmacist notation. The new process allowed them to save it (should it need to be designed later or required to follow), accept or reject and close the worksheet for final dispense to the patient.
CSP - ACCESS EXISTING WORKSHEET (RPH)
I constructed the following workflow that showed how a pharmacist could access an existing worksheet another pharmacist previously worked on; they could also continue working on this worksheet and remove, close, or add an exception for this prescription. In addition, access CSP history for this prescription to understand the previous pharmacist discussions about it and external audit purposes.
CSP - ACCESS EXISTING WORKSHEET (TECHNICIAN)
The last workflow I constructed showed how a technician could access an existing worksheet another technician or pharmacist previously worked on. In addition, they could continue working on this worksheet and save any required adjustments to the worksheet. A technician could not accept or reject a worksheet.
DESIGN
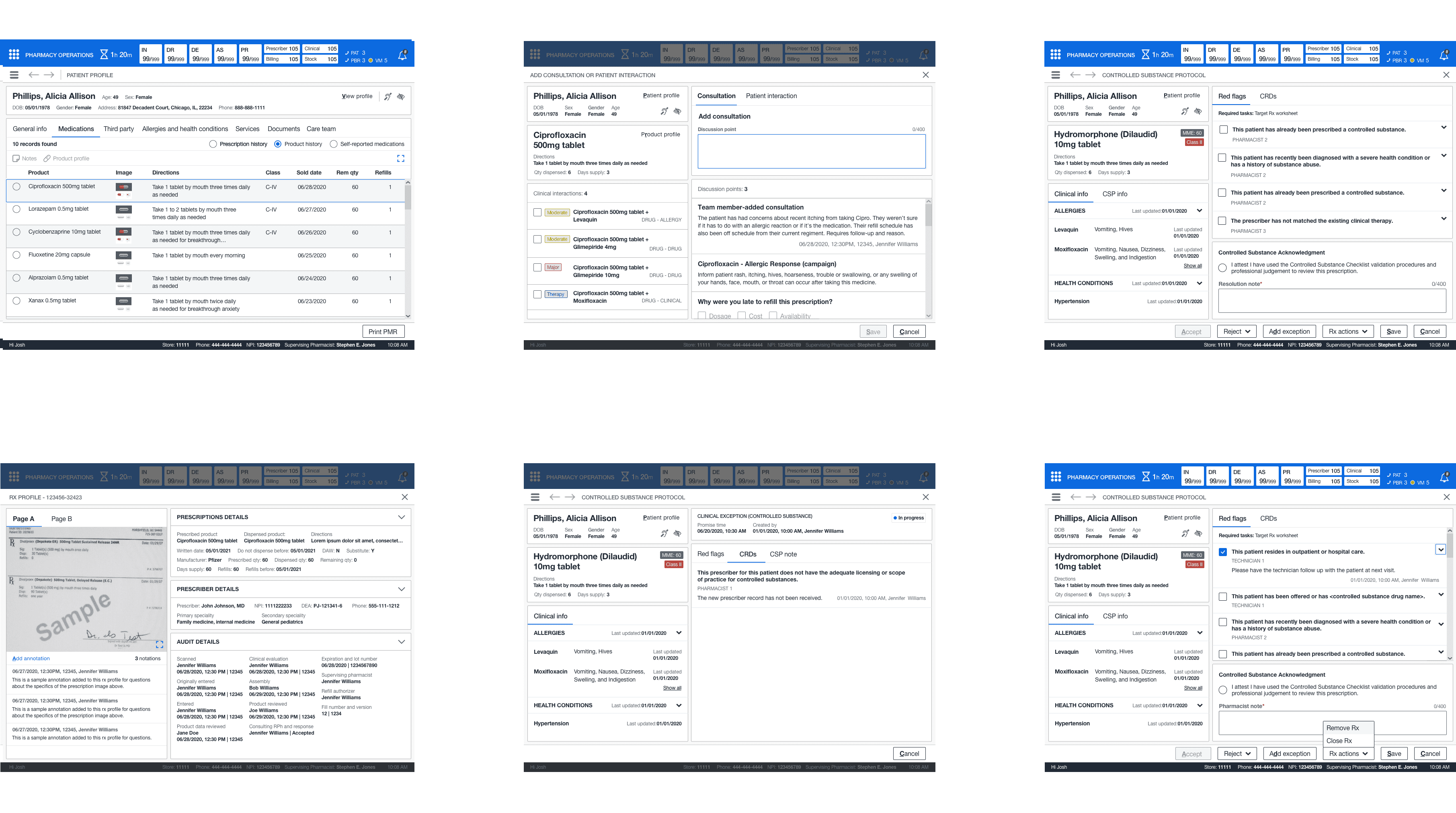
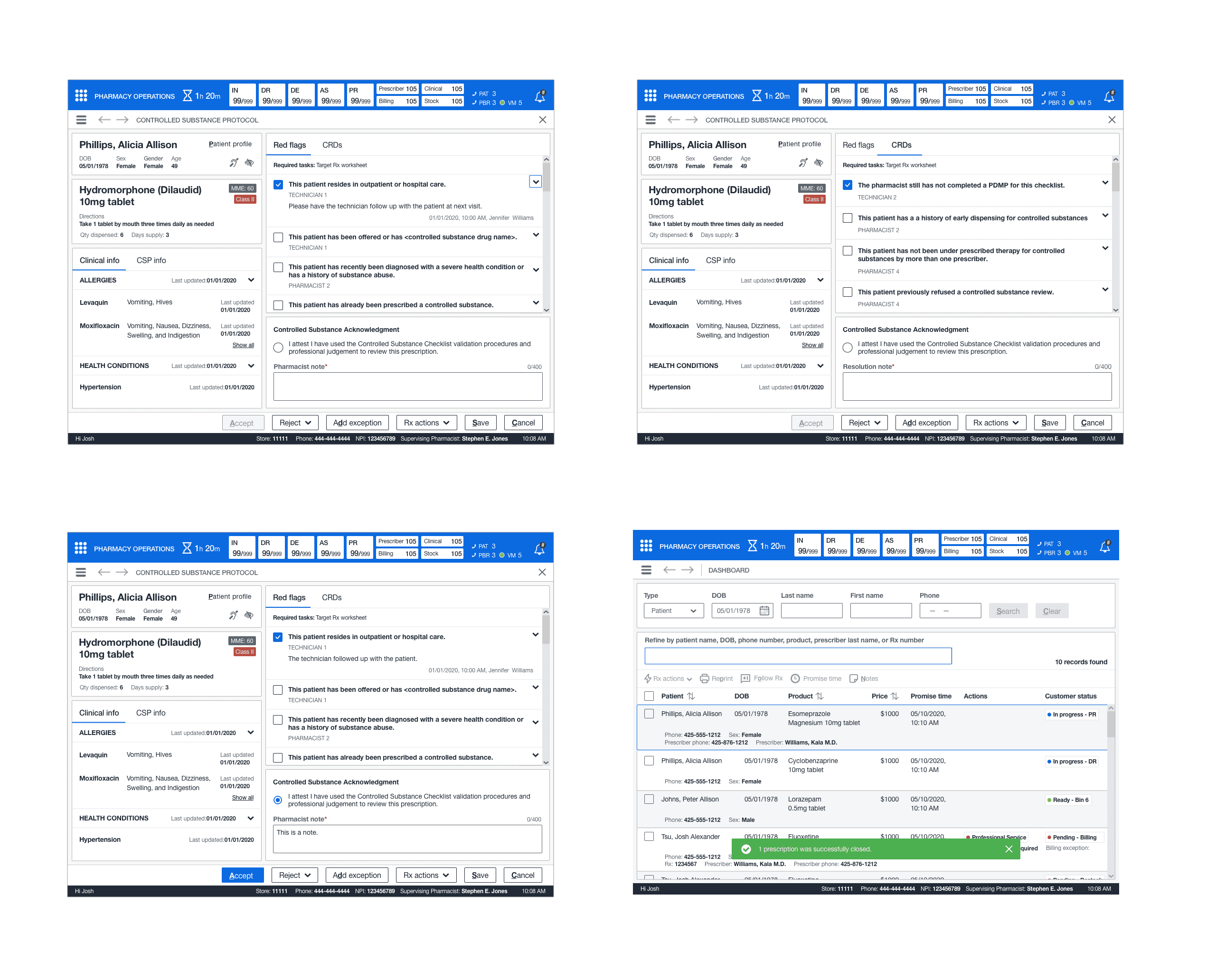
ACCESS OR COMPLETE AN EXISTING CSP WORKSHEET
This feature introduced the concept of eliminating duplicate processes for CSP prescriptions. Often, when a pharmacist or technician would log a worksheet’s red flags or CRDs, additional work or notations for the same prescription. At the same time, it didn’t result in incorrectly dispensed medications. The potential risk was due to the overlap and caused additional auditors to track intake to the point of sale. To alleviate this frustration, I worked with the PM and SME on defining the most commonly utilized red flags and CRDs.
ACCESS OR COMPLETE AN EXISTING
CSP WORKSHEET
This feature introduced the concept of eliminating duplicate processes for CSP prescriptions. Often, when a pharmacist or technician would log a worksheet’s red flags or CRDs, additional work or notations for the same prescription. At the same time, it didn’t result in incorrectly dispensed medications. The potential risk was due to the overlap and caused additional auditors to track intake to the point of sale. To alleviate this frustration, I worked with the PM and SME on defining the most commonly utilized red flags and CRDs.
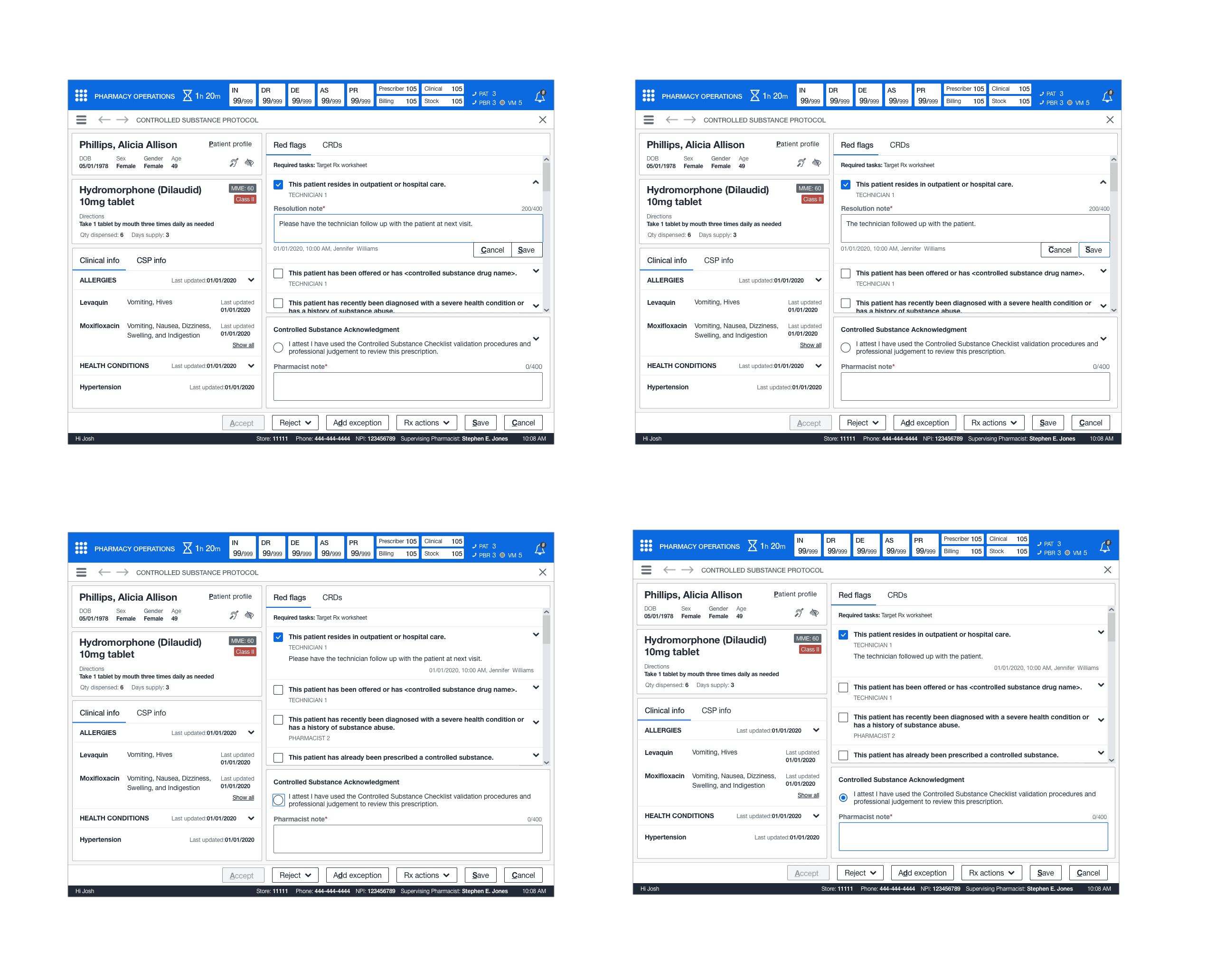
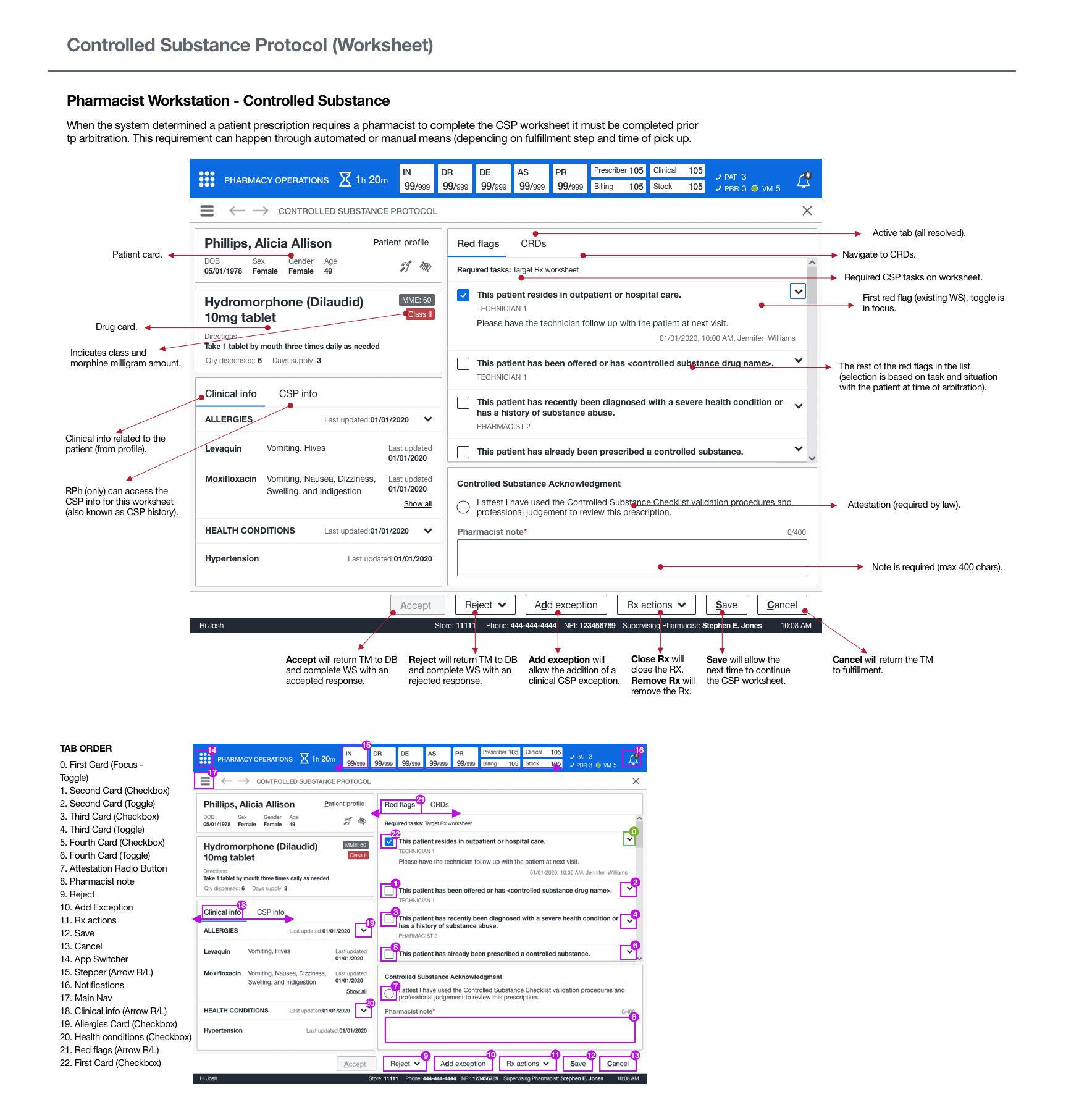
NOTATION
A pharmacist must have the ability to view and notate on technician and pharmacist red flags and CRDs. I designed a checklist format where a pharmacist could tab open either type and add a resolution note. Due to the limited availability of hotkeys, I introduced “Ctrl+Alt+S” to quickly save the note and “Ctrl+Alt+C” for cancel.
ACKNOWLEDGMENT
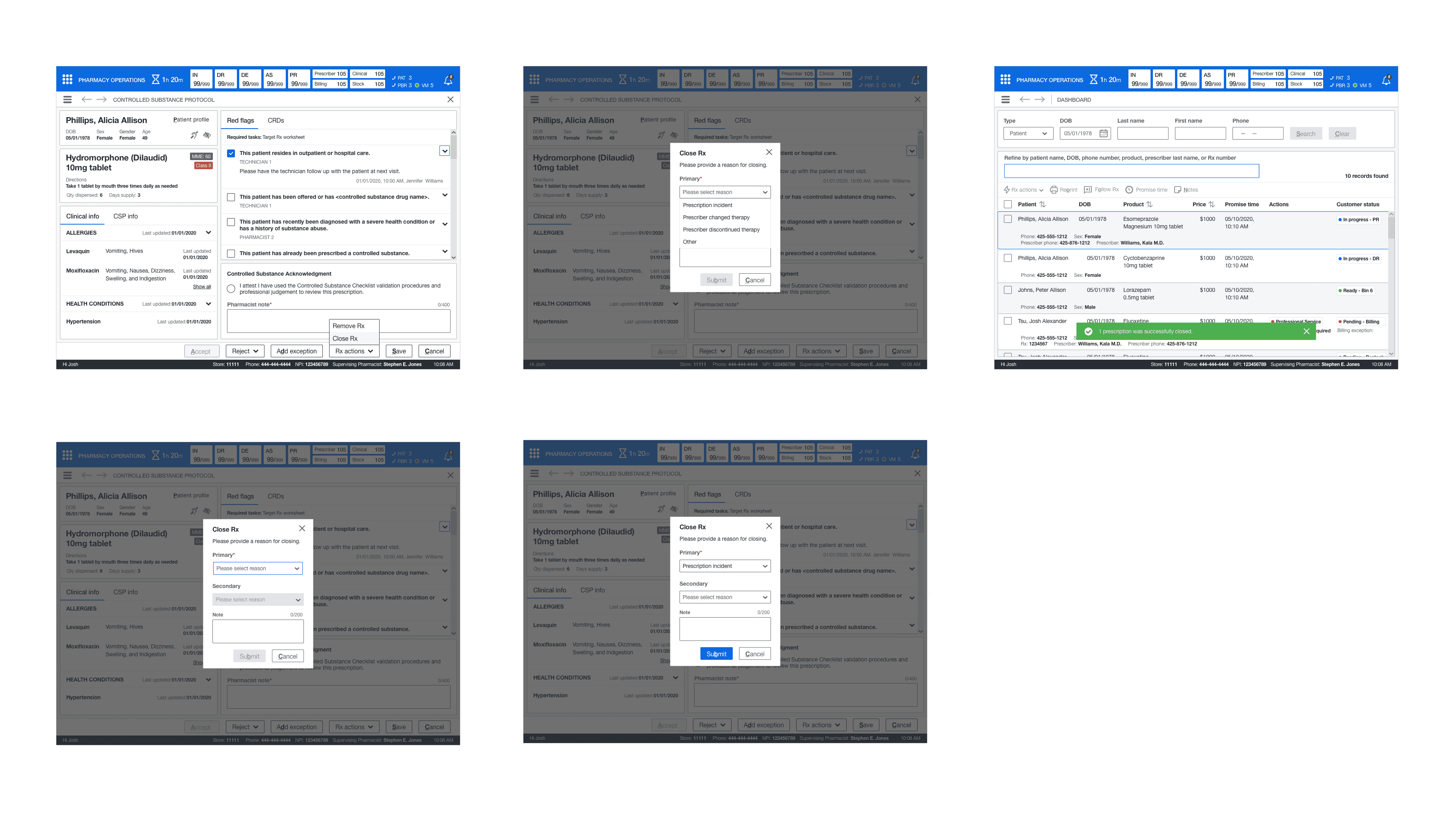
A pharmacist could complete their edits, acknowledge their attestation, and add their message. Next, they could either save the worksheet to have another team member work on it or accept and reject it for a specific reason. Depending on where the worksheet was completed in the process, it would return them after completing the worksheet (most commonly, they would be on the dashboard).
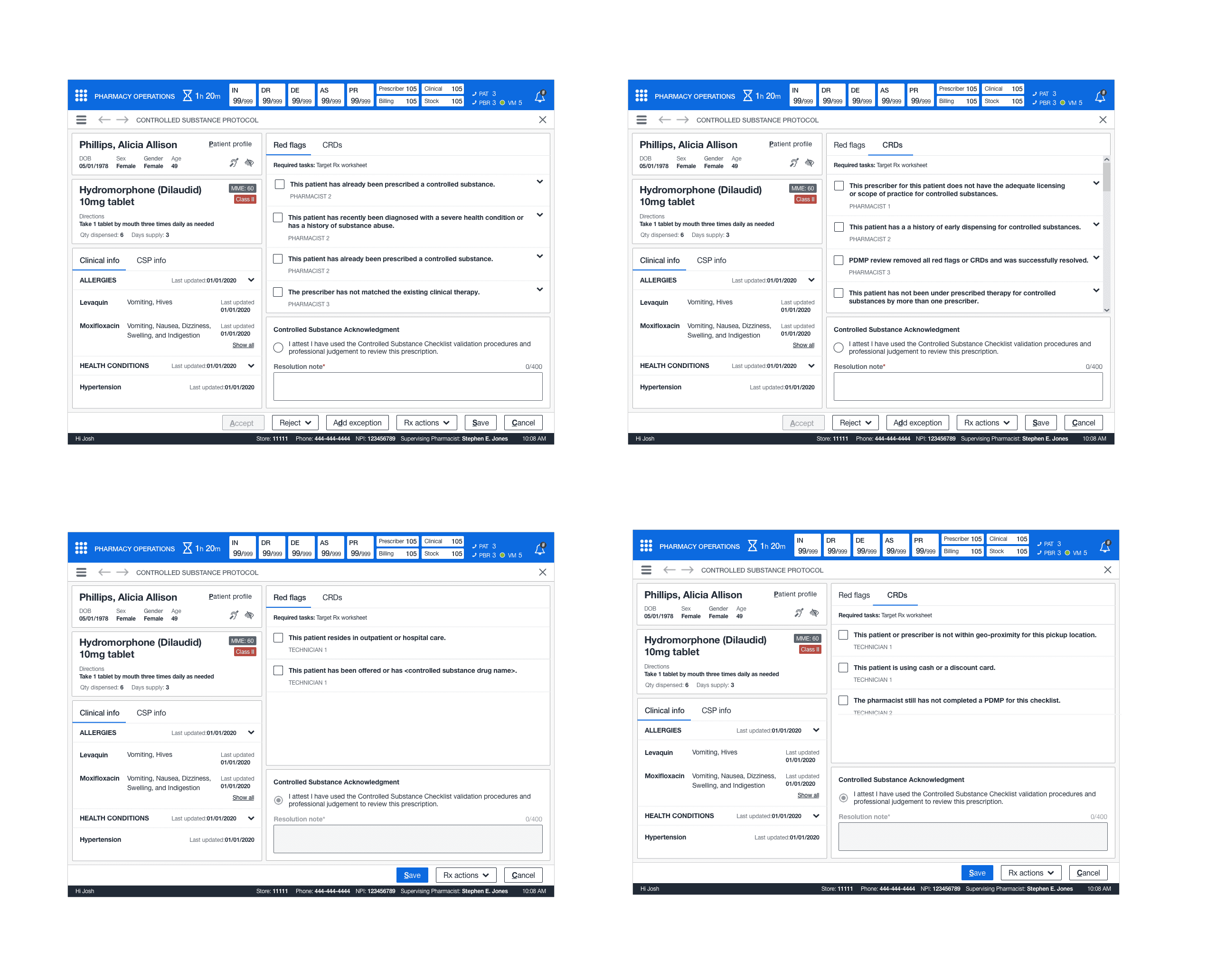
CREATE A NEW CSP WORKSHEET
This feature brought about the concept of removing offline worksheets entirely. Previously, team members had created a new worksheet if a CSP prescription did not have one, which often resulted in the team member making an unnecessary worksheet due to how cluttered the file was. To solve this, a pharmacy or team member could create a new worksheet if a CSP prescription required it and did not have one attached to it. They could perform all the standard functions needed on an new worksheet; however, new worksheets did not contain previous entries or information as it was new.
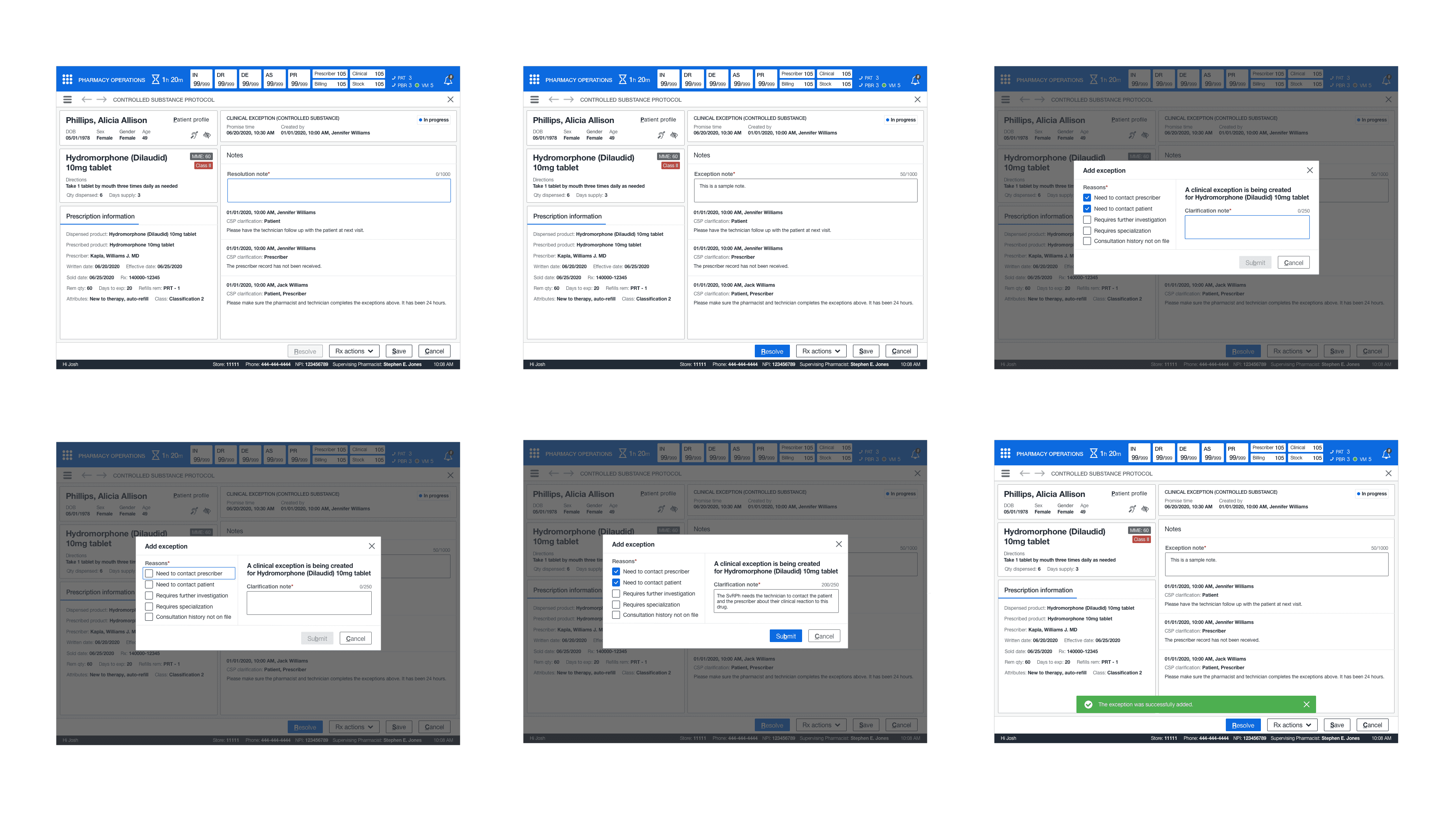
CREATE A NEW CLINICAL EXCEPTION FOR CSP WORKSHEET
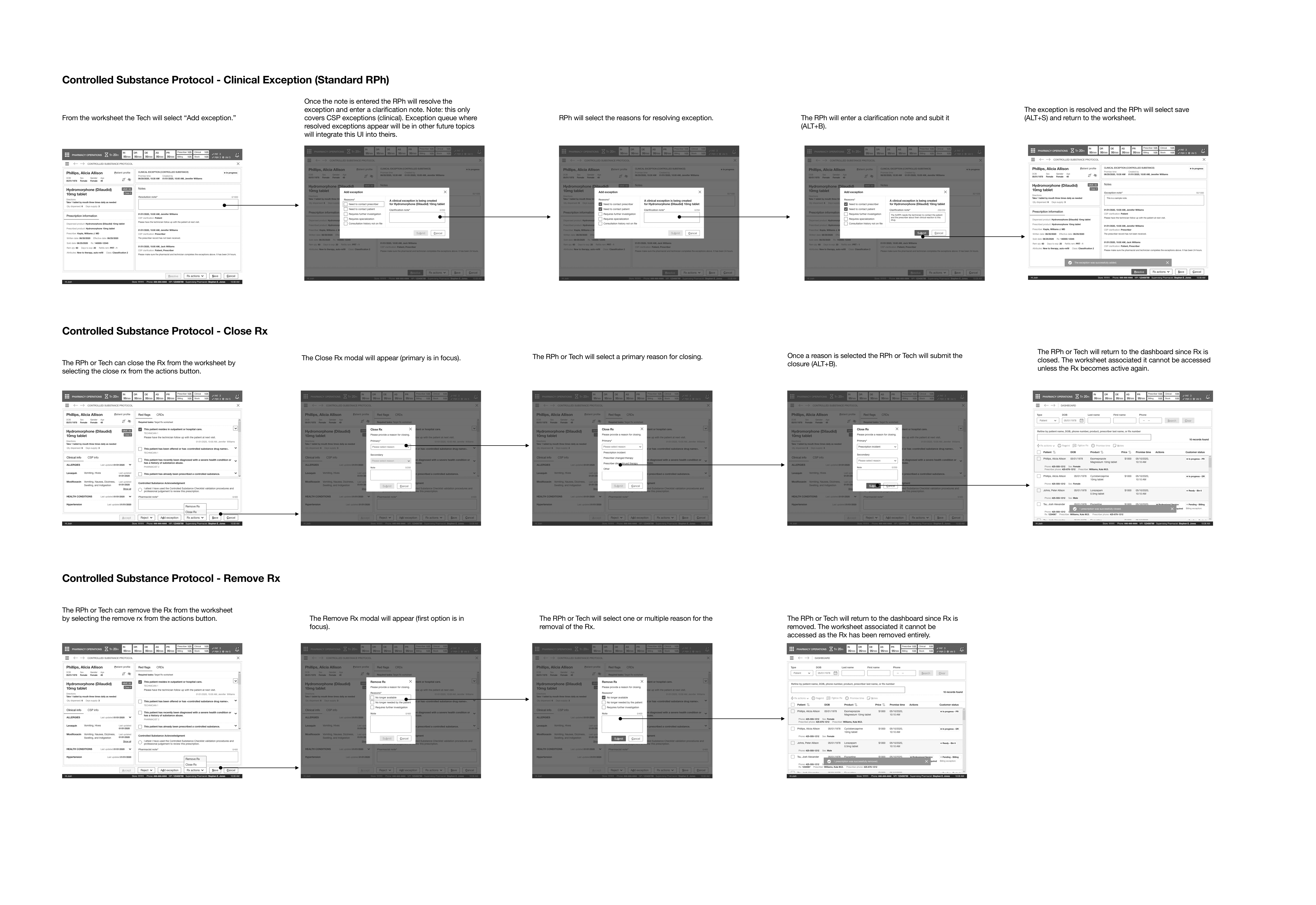
This feature extended the ability for a pharmacist to postpone a dispense for a CSP prescription through a clinical exception from a standard list of options. This new feature required me to design a base page for clinical exceptions, which contained all prescription info, previous notes, and the ability to resolve it from the exception queue depending on why it was added.
Clinical exceptions for CSP were immediate actions of add and resolve. Because of audit trail reasons to understand who added it, when and why, and resolved it. This prescription could contain notes from other team members who had previously added it to the queue and understand the history of this particular exception. Once the resolution note was entered, a pharmacist would resolve it by answering the simple prompt and returning to their point of origin (in this case, it was the CSP worksheet).
CREATE A NEW CLINICAL EXCEPTION
FOR CSP WORKSHEET
This feature extended the ability for a pharmacist to postpone a dispense for a CSP prescription through a clinical exception from a standard list of options. This new feature required me to design a base page for clinical exceptions, which contained all prescription info, previous notes, and the ability to resolve it from the exception queue depending on why it was added.
Clinical exceptions for CSP were immediate actions of add and resolve. Because of audit trail reasons to understand who added it, when and why, and resolved it. This prescription could contain notes from other team members who had previously added it to the queue and understand the history of this particular exception. Once the resolution note was entered, a pharmacist would resolve it by answering the simple prompt and returning to their point of origin (in this case, it was the CSP worksheet).
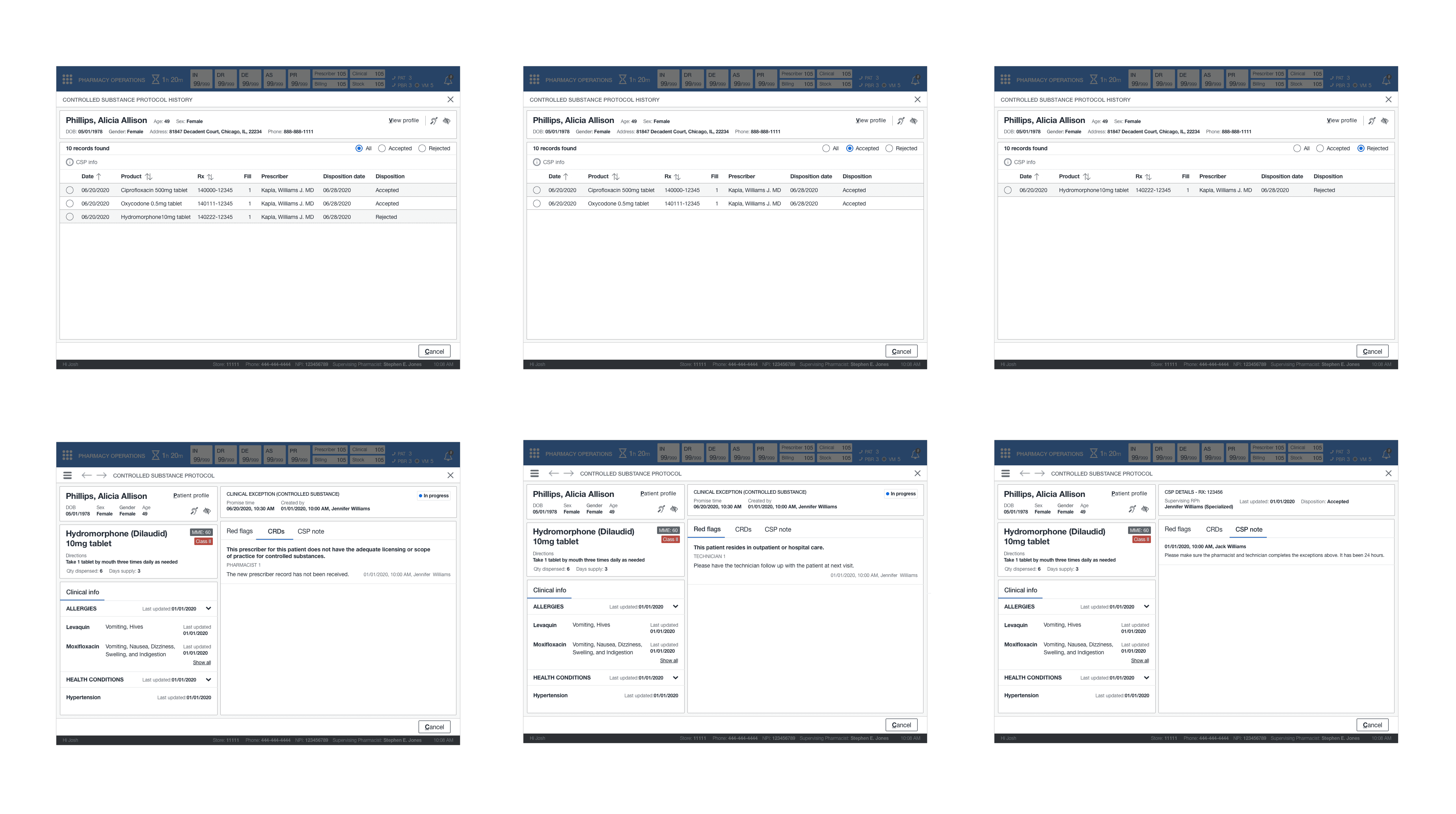
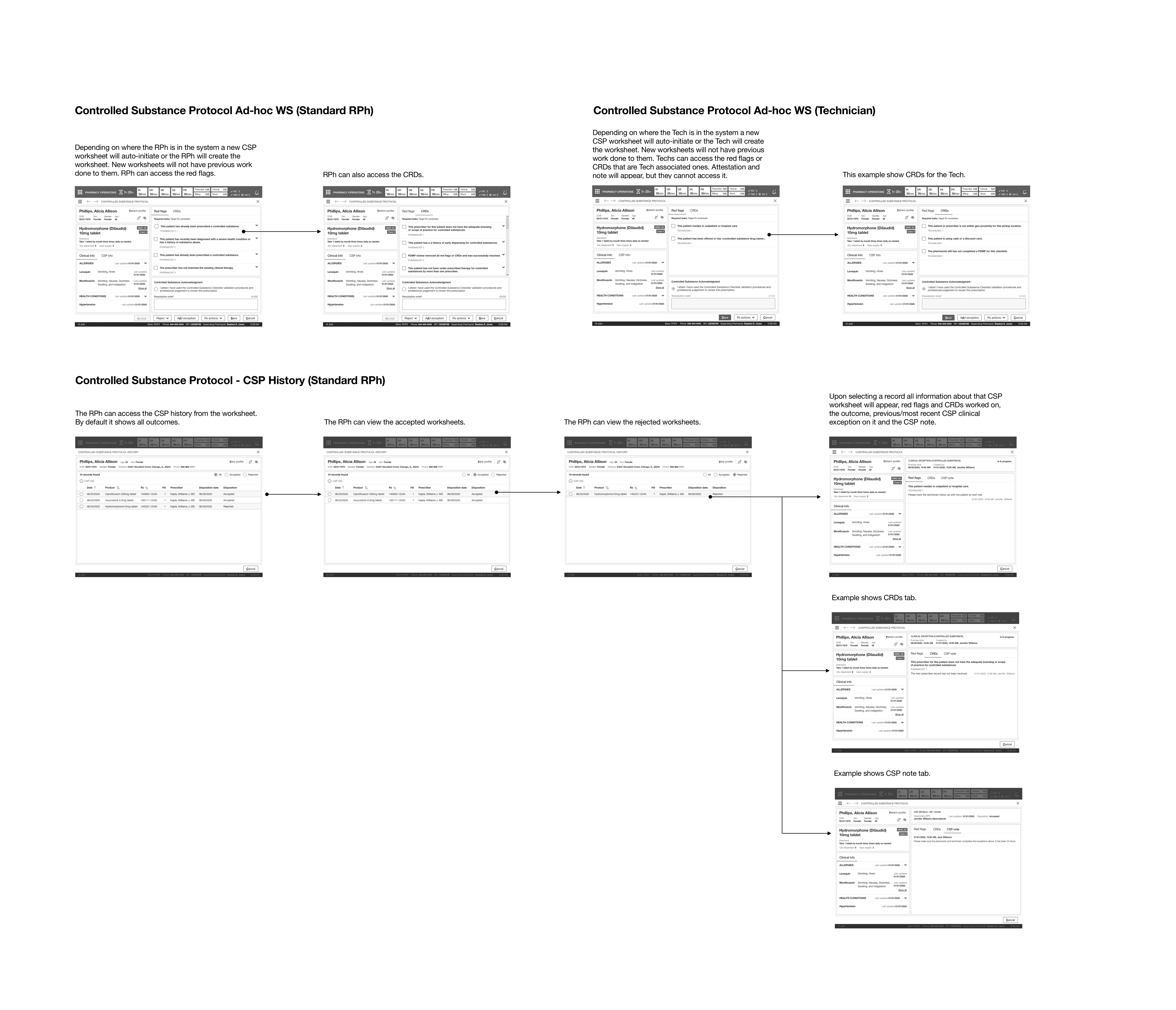
ACCESS CSP INFO (HISTORY) ON AN EXISTING WORKSHEET
This feature helped establish a documentation process for CSP prescriptions that drew team members away from their wayward thinking and processes. All interactions, outcomes, and notations were placed in a confusing folder procedure for patients' CSP prescriptions.
As there was no documentation process, I established one with the SME and stakeholders. I was able to align them on the documentation tied at the prescription level and contain all attestations, which CRDs or red flags were assigned to that record, and which pharmacist had worked on it and completed it.
Only pharmacists could access this information and readily do so while working on a worksheet if they needed to refer to it. All this information was read-only and established two new read-only patterns for this card format. In addition, it would show the clinical info at the time of resolution on previous worksheets.
ACCESS CSP INFO (HISTORY) ON AN
EXISTING WORKSHEET
This feature helped establish a documentation process for CSP prescriptions that drew team members away from their wayward thinking and processes. All interactions, outcomes, and notations were placed in a confusing folder procedure for patients' CSP prescriptions.
As there was no documentation process, I established one with the SME and stakeholders. I was able to align them on the documentation tied at the prescription level and contain all attestations, which CRDs or red flags were assigned to that record, and which pharmacist had worked on it and completed it.
Only pharmacists could access this information and readily do so while working on a worksheet if they needed to refer to it. All this information was read-only and established two new read-only patterns for this card format. In addition, it would show the clinical info at the time of resolution on previous worksheets.
CLOSE RX FROM CSP WORKSHEET (EXISTING OR NEW WORKSHEET)
This feature adopted the pattern and functionality from “Rx Info”. It gave a pharmacist or technician the ability to close a prescription if the patient no longer used the medication or if it was no longer available.
CLOSE RX FROM CSP WORKSHEET
(EXISTING OR NEW WORKSHEET)
This feature adopted the pattern and functionality from “Rx Info”. It gave a pharmacist or technician the ability to close a prescription if the patient no longer used the medication or if it was no longer available.
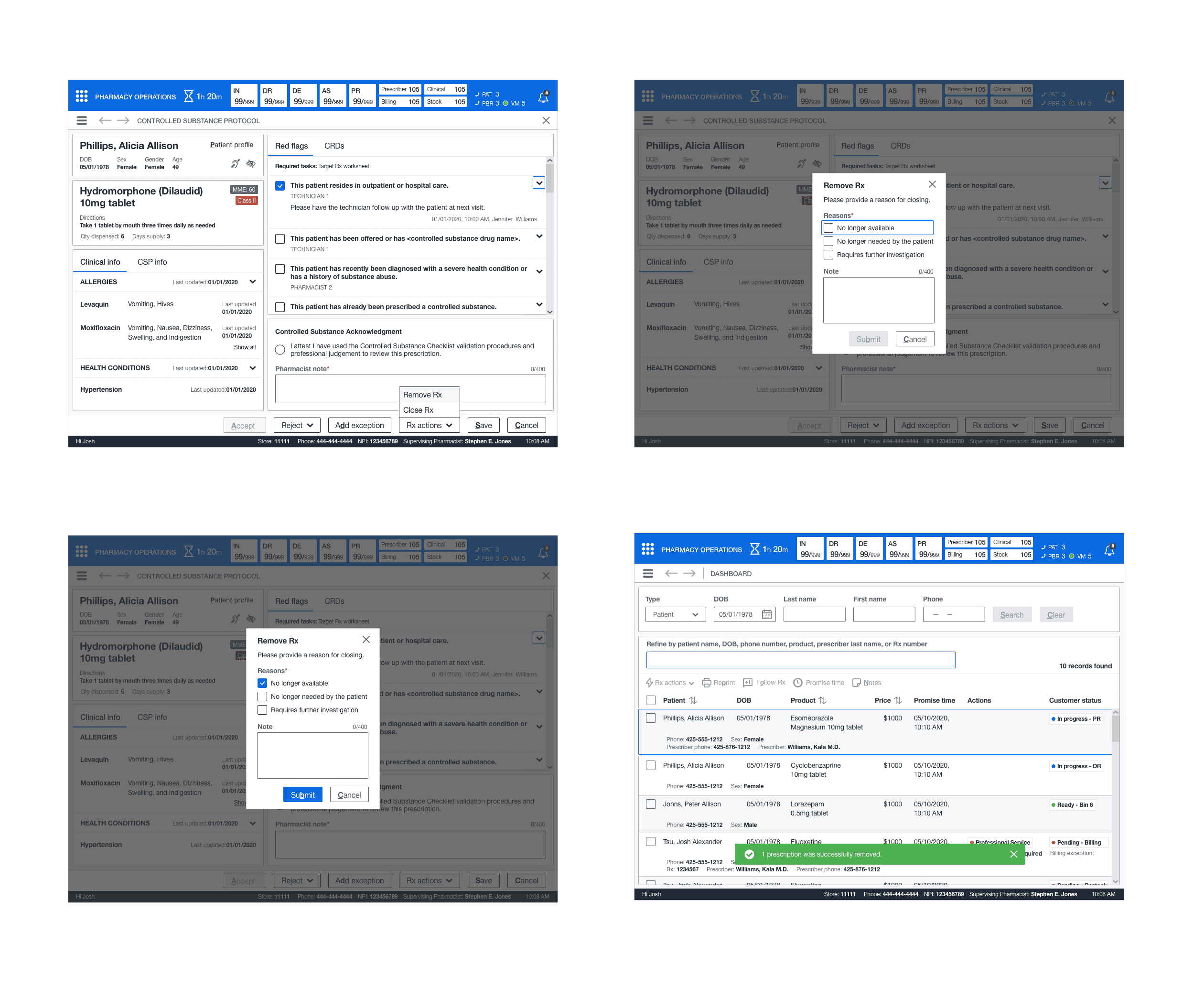
REMOVE RX FROM CSP WORKSHEET
(EXISTING OR NEW WORKSHEET)
This feature adopted Rx Info's "Close Rx" pattern and functionality. It gave a pharmacist or technician the ability to remove a prescription if the patient no longer used the medication, if it was no longer available, or required further investigation. This process would delete the prescription from the system entirely and place it in a purged folder (which the system would periodically flush).
THROWING A CURVEBALL
I completed the initial screen before storyboard construction when I was tasked with training and onboarding the new junior designer to design best practices and processes for handling topics. I brought them up to speed on stand-ups, office hours, and other internal functions. I was able to get them started reviewing the library and documentation process.
I brought them into the topic I was working on to show them the process and give them a hands-on experience. This approach was especially beneficial because it helped me test them to see if they asked questions and learn more about their design thinking and interest in the umbrella of design. While I trained this designer, I started constructing the storyboard.
STORYBOARD
Next, I constructed the wireframes into a storyboard that showed the paths for the defined use cases and scenarios for a pharmacist and a technician.
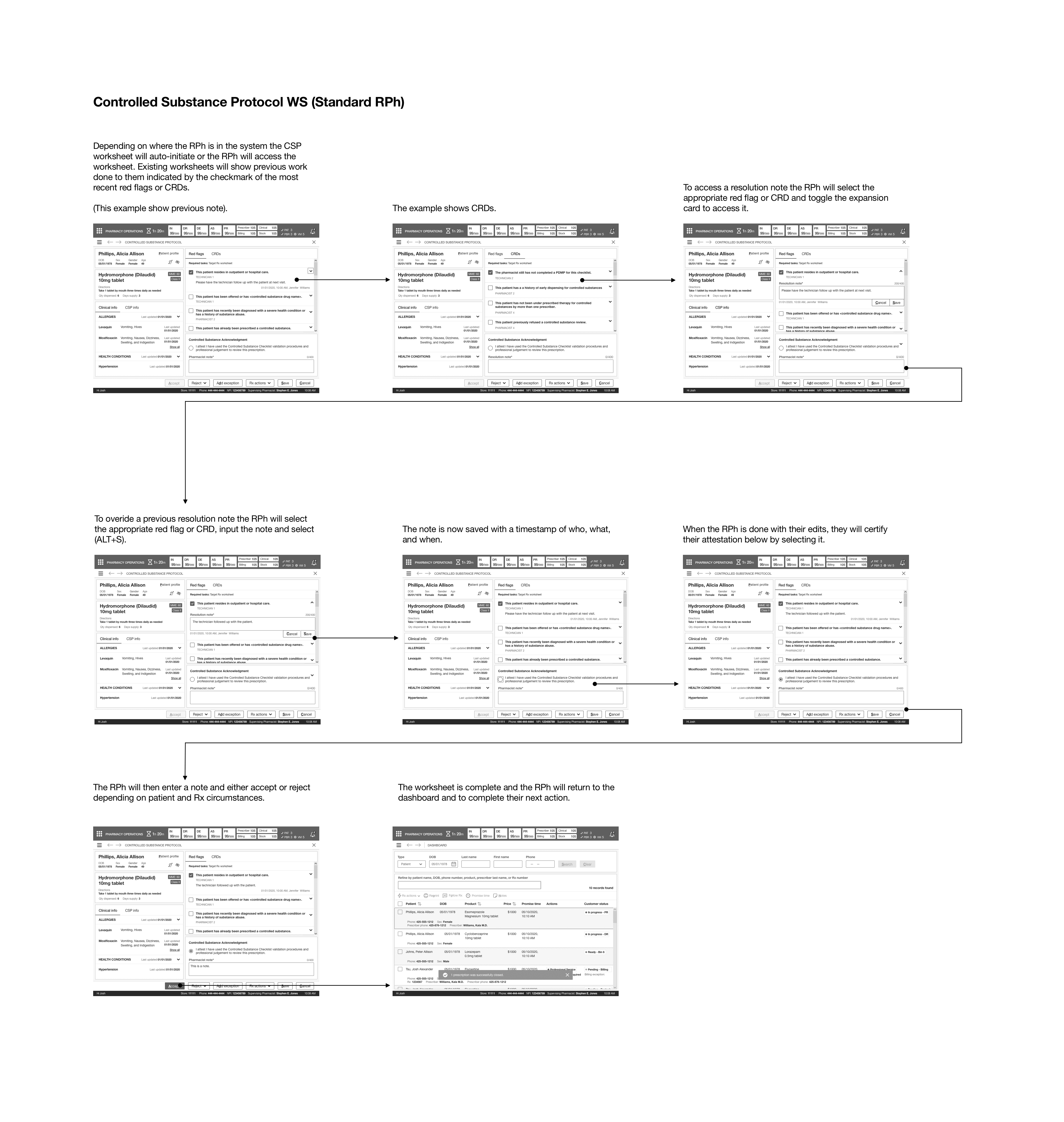
CSP WS (RPH)
This path showed how a pharmacist could access or complete an existing CSP worksheet. From this worksheet, they could make any edits to the CRDs or red flags, add a resolution note, and then complete their attestation. In addition, remove, close, or add a clinical exception to the prescription. Lastly, accept, reject to complete the worksheet or save the worksheet for a future continuation.
CSP AD-HOC WS (RPH/TECH)
This path showed how a pharmacist or technician could add a new worksheet to an existing or new CSP prescription. This task could be done during fulfillment but would most commonly be done from the pharmacy dashboard.
CSP - CLINICAL EXCEPTION (RPH)
This path showed how a pharmacist could add a clinical exception to the worksheet to prevent the point of sale and restart the fulfillment process for this CSP prescription based on the determined criteria for adding and resolving the exception.
CSP - CLOSE RX
This path showed how a pharmacist or technician could close a prescription from a worksheet for a CSP prescription.
CSP - REMOVE RX
This path showed how a pharmacist or technician could remove a prescription from a worksheet for a CSP prescription.
Once the storyboard was complete, the first review was scheduled. During this review, I was going to task the junior designer with taking notes and seeing how the design review process was done. In addition, I wanted them to understand more about the architecture and workflow of the system.
THE FIRST LEADERSHIP REVIEW
I set up the first review and introduced the junior designer to everyone as this designer was a new hire. I explained that the designer would be sitting at the meeting to understand the process and take notes. The first review would cover some features. I first went through the screens for how a pharmacist could access or complete an existing worksheet and showed the difference between new and existing worksheets.
Next, I explained our process for structuring the CRDs and red flags for each team member and clarified that a technician could not access history, complete a worksheet, or add resolution notes. Only that they could work on their set CRDs or red flags. The adverse being a pharmacist could access any of the CRDs/red flags, set a resolution, and it would require an attestation to their final comment when accepting or rejecting a worksheet.
FINAL CLARIFICATION
The next series of the screen I reviewed with the leadership team was the CSP history. I explained the functionality behind accessing previous CSP information and outcomes that the last pharmacist had interacted on. I explained how it notates the red flags and CRDs tied to it, the note, and the result. The information could be accessed at the prescription level. The leadership team was happy with the presentation and had no feedback to implement. They did ask to see a complete list of CRDs and red flags once the fulfillment team fully defined them.


THE SECOND LEADERSHIP REVIEW
For the second review, I continued with the add exception screens. Exception queue functionality would be visited in a future topic. I showcased the initial base functionality of the screen I designed and explained how to add and resolve the exception in an instantaneous interaction. Post-resolution resulted in the prescription returning the beginning of the funnel process for the medications.
Their feedback was to make sure clinical exception functionality was incorporated into the future topic, and we connected with that team on feasibility and continuity within the system. The last set of screens I went over was closing a prescription, which did not have any feedback, and then removing a drug, which also did not have any input to implement, only clarifications on the system purge of the prescription.
DETAILED DESIGN
As I did with the previous topic, I utilized the design library to make pixel-perfect mockups of the core screens. I first completed the pharmacist screens and then the technician screens. While working on screens, I had the junior designer follow me on the screen to understand the process for implementing new patterns and how the master file worked and learn to use the library more in-depth. Once the detailed design was complete, I took the completed screens and started the annotations and tab order.
ANNOTATIONS AND TAB ORDER
I created annotated wireframes and tab orders for all screens. These artifacts would aid engineers, and technical architects in understanding the functionality and act as a blueprint for elaboration. Once I completed these artifacts, the executive leadership had an offline review, and they signed off on the UX. The offline check consisted of reviewing all annotated wireframes and Confluence docs.
DESIGN
ACCESS OR COMPLETE AN EXISTING CSP WORKSHEET
This feature introduced the concept of eliminating duplicate processes for CSP prescriptions. Often, when a pharmacist or technician would log a worksheet’s red flags or CRDs, additional work or notations for the same prescription. At the same time, it didn’t result in incorrectly dispensed medications. The potential risk was due to the overlap and caused additional auditors to track intake to the point of sale. To alleviate this frustration, I worked with the PM and SME on defining the most commonly utilized red flags and CRDs.
NOTATION
A pharmacist must have the ability to view and notate on technician and pharmacist red flags and CRDs. I designed a checklist format where a pharmacist could tab open either type and add a resolution note. Due to the limited availability of hotkeys, I introduced “Ctrl+Alt+S” to quickly save the note and “Ctrl+Alt+C” for cancel.
ACKNOWLEDGMENT
A pharmacist could complete their edits, acknowledge their attestation, and add their message. Next, they could either save the worksheet to have another team member work on it or accept and reject it for a specific reason. Depending on where the worksheet was completed in the process, it would return them after completing the worksheet (most commonly, they would be on the dashboard).
CREATE A NEW CSP WORKSHEET
This feature brought about the concept of removing offline worksheets entirely. Previously, team members had created a new worksheet if a CSP prescription did not have one, which often resulted in the team member making an unnecessary worksheet due to how cluttered the file was. To solve this, a pharmacy or team member could create a new worksheet if a CSP prescription required it and did not have one attached to it. They could perform all the standard functions needed on an new worksheet; however, new worksheets did not contain previous entries or information as it was new.
CREATE A NEW CLINICAL EXCEPTION FOR CSP WORKSHEET
This feature extended the ability for a pharmacist to postpone a dispense for a CSP prescription through a clinical exception from a standard list of options. This new feature required me to design a base page for clinical exceptions, which contained all prescription info, previous notes, and the ability to resolve it from the exception queue depending on why it was added.
Clinical exceptions for CSP were immediate actions of add and resolve. Because of audit trail reasons to understand who added it, when and why, and resolved it. This prescription could contain notes from other team members who had previously added it to the queue and understand the history of this particular exception. Once the resolution note was entered, a pharmacist would resolve it by answering the simple prompt and returning to their point of origin (in this case, it was the CSP worksheet).
ACCESS CSP INFO (HISTORY) ON AN EXISTING WORKSHEET
This feature helped establish a documentation process for CSP prescriptions that drew team members away from their wayward thinking and processes. All interactions, outcomes, and notations were placed in a confusing folder procedure for patients' CSP prescriptions.
As there was no documentation process, I established one with the SME and stakeholders. I was able to align them on the documentation tied at the prescription level and contain all attestations, which CRDs or red flags were assigned to that record, and which pharmacist had worked on it and completed it.
Only pharmacists could access this information and readily do so while working on a worksheet if they needed to refer to it. All this information was read-only and established two new read-only patterns for this card format. In addition, it would show the clinical info at the time of resolution on previous worksheets.
CLOSE RX FROM CSP WORKSHEET (EXISTING OR NEW WORKSHEET)
This feature adopted the pattern and functionality from “Rx Info”. It gave a pharmacist or technician the ability to close a prescription if the patient no longer used the medication or if it was no longer available.
REMOVE RX FROM CSP WORKSHEET
(EXISTING OR NEW WORKSHEET)
This feature adopted Rx Info's "Close Rx" pattern and functionality. It gave a pharmacist or technician the ability to remove a prescription if the patient no longer used the medication, if it was no longer available, or required further investigation. This process would delete the prescription from the system entirely and place it in a purged folder (which the system would periodically flush).
THROWING A CURVEBALL
I completed the initial screen before storyboard construction when I was tasked with training and onboarding the new junior designer to design best practices and processes for handling topics. I brought them up to speed on stand-ups, office hours, and other internal functions. I was able to get them started reviewing the library and documentation process.
I brought them into the topic I was working on to show them the process and give them a hands-on experience. This approach was especially beneficial because it helped me test them to see if they asked questions and learn more about their design thinking and interest in the umbrella of design. While I trained this designer, I started constructing the storyboard.
STORYBOARD
Next, I constructed the wireframes into a storyboard that showed the paths for the defined use cases and scenarios for a pharmacist and a technician.
CSP WS (RPH)
This path showed how a pharmacist could access or complete an existing CSP worksheet. From this worksheet, they could make any edits to the CRDs or red flags, add a resolution note, and then complete their attestation. In addition, remove, close, or add a clinical exception to the prescription. Lastly, accept, reject to complete the worksheet or save the worksheet for a future continuation.
CSP AD-HOC WS (RPH/TECH)
This path showed how a pharmacist or technician could add a new worksheet to an existing or new CSP prescription. This task could be done during fulfillment but would most commonly be done from the pharmacy dashboard.
CSP - CLINICAL EXCEPTION (RPH)
This path showed how a pharmacist could add a clinical exception to the worksheet to prevent the point of sale and restart the fulfillment process for this CSP prescription based on the determined criteria for adding and resolving the exception.
CSP - CLOSE RX
This path showed how a pharmacist or technician could close a prescription from a worksheet for a CSP prescription.
CSP - REMOVE RX
This path showed how a pharmacist or technician could remove a prescription from a worksheet for a CSP prescription.
Once the storyboard was complete, the first review was scheduled. During this review, I was going to task the junior designer with taking notes and seeing how the design review process was done. In addition, I wanted them to understand more about the architecture and workflow of the system.
THE FIRST LEADERSHIP REVIEW
I set up the first review and introduced the junior designer to everyone as this designer was a new hire. I explained that the designer would be sitting at the meeting to understand the process and take notes. The first review would cover some features. I first went through the screens for how a pharmacist could access or complete an existing worksheet and showed the difference between new and existing worksheets.
Next, I explained our process for structuring the CRDs and red flags for each team member and clarified that a technician could not access history, complete a worksheet, or add resolution notes. Only that they could work on their set CRDs or red flags. The adverse being a pharmacist could access any of the CRDs/red flags, set a resolution, and it would require an attestation to their final comment when accepting or rejecting a worksheet.
FINAL CLARIFICATION
The next series of the screen I reviewed with the leadership team was the CSP history. I explained the functionality behind accessing previous CSP information and outcomes that the last pharmacist had interacted on. I explained how it notates the red flags and CRDs tied to it, the note, and the result. The information could be accessed at the prescription level. The leadership team was happy with the presentation and had no feedback to implement. They did ask to see a complete list of CRDs and red flags once the fulfillment team fully defined them.
THE SECOND LEADERSHIP REVIEW
For the second review, I continued with the add exception screens. Exception queue functionality would be visited in a future topic. I showcased the initial base functionality of the screen I designed and explained how to add and resolve the exception in an instantaneous interaction. Post-resolution resulted in the prescription returning the beginning of the funnel process for the medications.
Their feedback was to make sure clinical exception functionality was incorporated into the future topic, and we connected with that team on feasibility and continuity within the system. The last set of screens I went over was closing a prescription, which did not have any feedback, and then removing a drug, which also did not have any input to implement, only clarifications on the system purge of the prescription.
DETAILED DESIGN
As I did with the previous topic, I utilized the design library to make pixel-perfect mockups of the core screens. I first completed the pharmacist screens and then the technician screens. While working on screens, I had the junior designer follow me on the screen to understand the process for implementing new patterns and how the master file worked and learn to use the library more in-depth. Once the detailed design was complete, I took the completed screens and started the annotations and tab order.
ANNOTATIONS AND TAB ORDER
I created annotated wireframes and tab orders for all screens. These artifacts would aid engineers, and technical architects in understanding the functionality and act as a blueprint for elaboration. Once I completed these artifacts, the executive leadership had an offline review, and they signed off on the UX. The offline check consisted of reviewing all annotated wireframes and Confluence docs.
NEXT STEPS
ELABORATION
The next step was to have elaboration scheduled to clarify any outstanding questions or concerns. Then, I described the rest of the functionality, including the hotkey and confirmation of tab order. Finally, I explained all questions with the elaboration teams and then moved on to my next topic.
NEXT STEPS
ELABORATION
The next step was to have elaboration scheduled to clarify any outstanding questions or concerns. Then, I described the rest of the functionality, including the hotkey and confirmation of tab order. Finally, I explained all questions with the elaboration teams and then moved on to my next topic.
OUTCOMES
imrpoved method
The new CSP verification method made the pharmacy team's process smooth and simple, allowing them to fully transition away from their legacy system and offline methods. Additionally, it nearly eliminated duplicate records from edits made by technicians or pharmacists.
EFFECTIVE MENTORING
The junior designer I mentored gained a strong understanding of the design system and process. Additionally, the time I spent mentoring other designers did not detract from my ability to fulfill my other design responsibilities.
OUTCOMES
imrpoved method
The new CSP verification method made the pharmacy team's process smooth and simple, allowing them to fully transition away from their legacy system and offline methods. Additionally, it nearly eliminated duplicate records from edits made by technicians or pharmacists.
EFFECTIVE MENTORING
The junior designer I mentored gained a strong understanding of the design system and process. Additionally, the time I spent mentoring other designers did not detract from my ability to fulfill my other design responsibilities.
LEARNINGS
RISK AND IMPACT
I learned how key this process was in ensuring that a patient’s prescription was correctly dispensed, especially even a CSP type. A pharmacist could lose their license and face heavy fines if a controlled substance was incorrectly administered to a patient, not to mention concern around substance abuse or potential addiction. It was pleasing to see how caring these pharmaceutical professionals are when it especially comes to this practice.
AMOUNT OF WORK
Pharmacists undergo rigorous training and process to ensure controlled substances are correctly dispensed. Unfortunately, this resulted in overlap and redundant work between pharmacy members. With the new feature in place, this would reduce or remove that overlap, but for every single new dispense for each CSP prescription, it would always require a worksheet.
LEARNINGS
RISK AND IMPACT
I learned how key this process was in ensuring that a patient’s prescription was correctly dispensed, especially even a CSP type. A pharmacist could lose their license and face heavy fines if a controlled substance was incorrectly administered to a patient, not to mention concern around substance abuse or potential addiction. It was pleasing to see how caring these pharmaceutical professionals are when it especially comes to this practice.
AMOUNT OF WORK
Pharmacists undergo rigorous training and process to ensure controlled substances are correctly dispensed. Unfortunately, this resulted in overlap and redundant work between pharmacy members. With the new feature in place, this would reduce or remove that overlap, but for every single new dispense for each CSP prescription, it would always require a worksheet.